

Managing Knee Arthritis
Knee Arthritis Relief Starts Here
Learn what causes knee arthritis pain and explore proven treatment options including exercise, braces, supplements, injections, and when surgery may help.
Living with knee pain can be frustrating—but effective treatment options exist.
Whether your symptoms are mild or more advanced, many patients improve with the right combination of exercise, weight loss, bracing, supplements, injections, or surgery when needed. Use this page to gain knowledge about arthritis, to explore your options and learn what may treatments may work best for you.
Common Non-Surgical Treatments
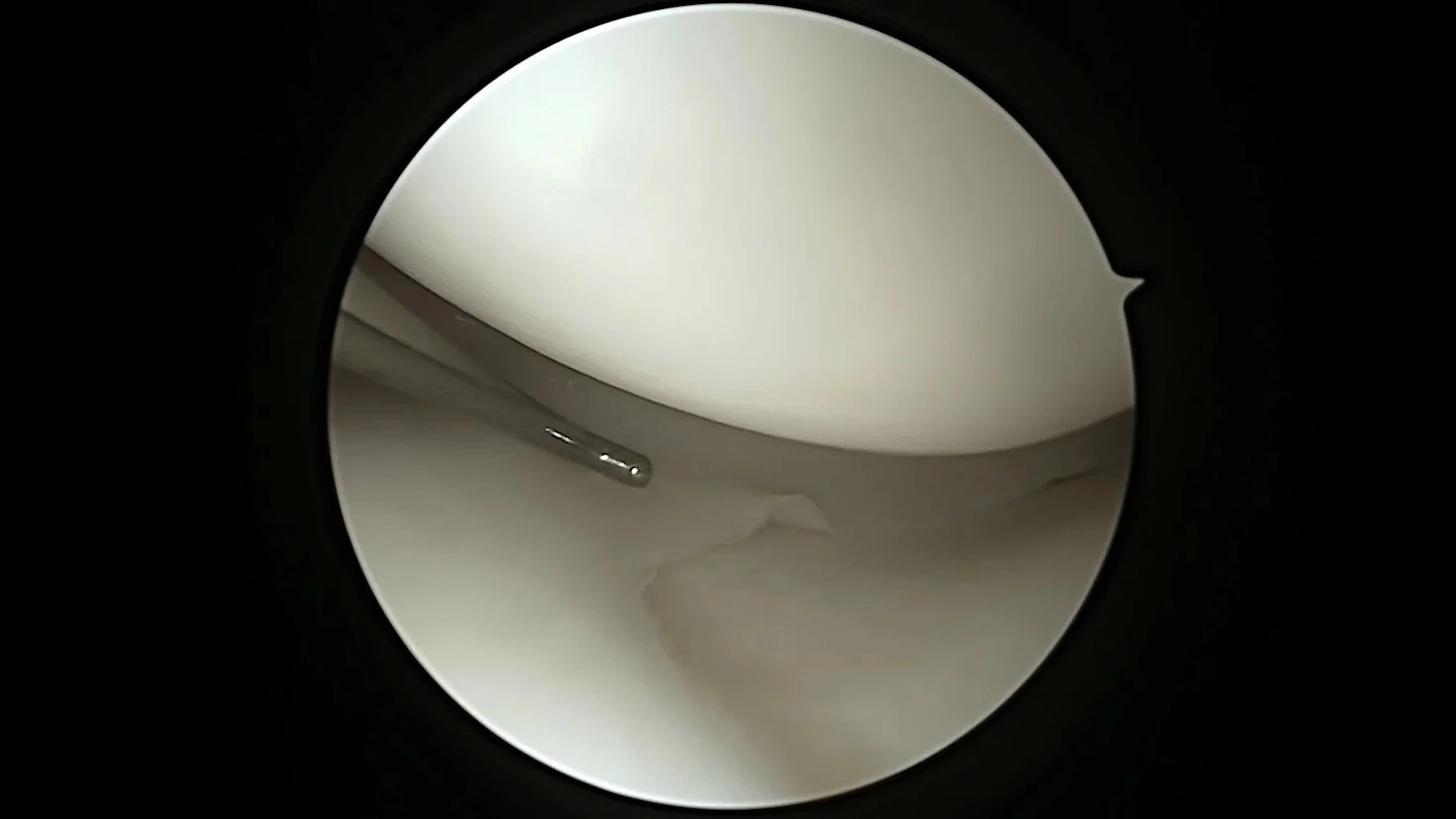
Normal appearing articular cartilage
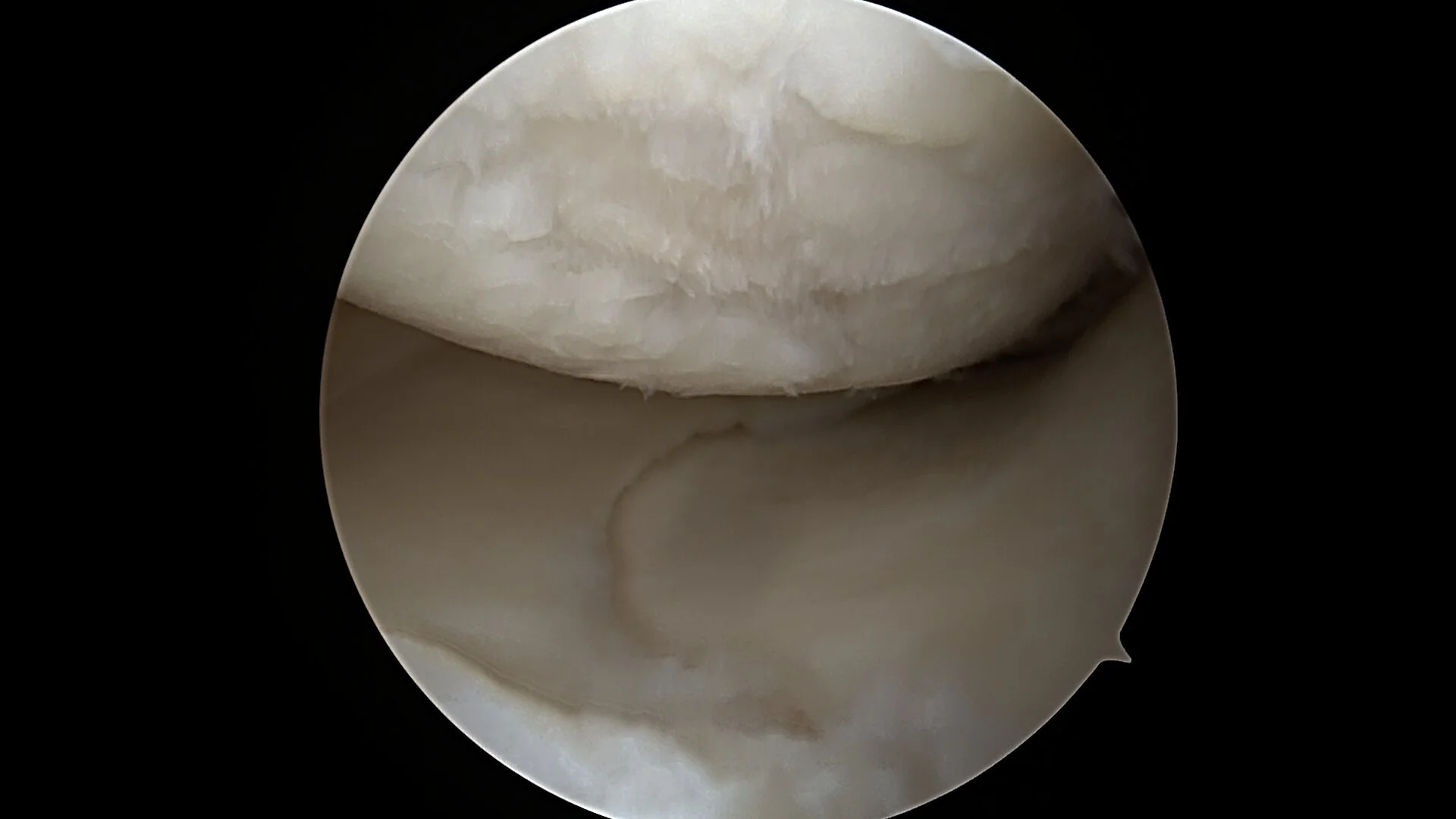
Appearance of Degenerative joint Disease Cartilage wear with uneven surfaces
WHAT IS ARTHRITIS?
Millions of people are affected by osteoarthritis (OA), also called degenerative joint disease (DJD). When it involves the knee, it is one of the most common causes of pain, stiffness, and loss of function.
Many patients hear the term “degenerative changes” but are left wondering what is actually degenerating. In knee osteoarthritis, the problem is the gradual loss of articular cartilage—the smooth, rubber-like tissue that covers the ends of the bones in the joint and allows them to glide smoothly with movement.
At the end of growth, this cartilage is thick and healthy. Over time, however, it can wear down or become damaged. Once cartilage is lost, the joint becomes less smooth, more irritated, and increasingly painful. In some cases, this process happens slowly with aging, and in others it may be accelerated by injury or mechanical stress..
Common contributors to knee degenerative joint disease include:
Genetics – A family history of arthritis can increase your risk.
Trauma or injury – Prior injuries can trigger changes that lead to gradual cartilage breakdown over time.
Malalignment – Being bow-legged or knock-kneed can place uneven pressure on the knee joint, accelerating wear.
Nutritional factors – Some studies suggest that deficiencies, such as low vitamin D, may play a role in joint health, though the relationship is not fully understood.
Meniscus tears – Damage to the meniscus reduces the knee’s natural shock absorption, increasing stress on cartilage and contributing to arthritis progression

Knee Xray appearance of bone-on-bone arthritis of the knee on the right side of the image.
WHY DOES DEGENERATIVE JOINT DISEASE HURT?
Degenerative joint disease causes pain through several overlapping mechanisms.
As cartilage wears away, the normally smooth joint surface becomes rough and uneven, increasing friction during movement.
Less cartilage leads to Increased stress on the underlying bone.
Increased bone stress can lead to bone marrow irritation/inflammation and occasionally microfractures
The Lining of the joint (synovium) often becomes inflammed in a process called synovitis
Over time, these combined sources of pain—cartilage loss, bone stress, and inflammation—lead to the progressive symptoms patients experience.

Exercise: One of the Most Effective Treatments for Knee Arthritis
Many patients are surprised to learn that the right exercise program is often one of the best ways to reduce knee arthritis pain.
Strengthening the muscles around the knee—especially the quadriceps, hips, and glutes—can decrease stress on the joint, improve stability, and make everyday activities easier.
Low-impact movement also helps reduce stiffness, improve motion, and keep the knee healthier over time.
The key is choosing the right exercises and progressing gradually.
Exercises That Often Help
Strengthening
Straight leg raises
Sit-to-stand squats
Step-ups
Glute bridges
Low Impact Cardio
Walking
Cycling
Pool exercise
Elliptical
Mobility
Gentle stretching
Yoga
Benefits of Exercise
✔ Reduces pain
✔ Improves walking and stairs
✔ Increases strength and stability
✔ Helps delay more invasive treatment

Worried Exercise Will “Wear Out” Your Knee?
This is a common concern. In most cases, appropriate exercise does not damage the knee. In fact, inactivity often leads to more weakness, stiffness, and pain.
Weight Loss: One of the Most Powerful Treatments for Knee Arthritis
Extra body weight places significant stress on the knee joint with every step. Even modest weight loss can reduce pain, improve walking, and make exercise easier.
Many patients tell me they want to lose weight but feel unable to exercise because of knee pain. The good news is that weight loss does not need to begin with intense workouts. For most people, nutrition changes are the most important first step.
As pain improves, activity often becomes easier—and progress can build from there.
Anti-Inflammatory Nutrition May Help Symptoms
Some foods may contribute to inflammation, while others may help support overall health and symptom control.
Focus More On:
✔ Lean proteins (chicken, fish, Greek yogurt, eggs)
✔ Vegetables and fruit
✔ Beans / legumes
✔ Olive oil
✔ Nuts and seeds
✔ Whole grains (if tolerated)
✔ Omega-3 rich fish (salmon, sardines)
Limit More Often:
✔ Sugary drinks
✔ Processed snacks
✔ Fast food
✔ Frequent fried foods
✔ Excess alcohol
✔ Highly processed carbohydrates
“I Can’t Exercise, So I Can’t Lose Weight.”
This is a very common belief—but not true.
Weight loss is often driven more by nutrition habits than formal exercise. Even if walking is limited right now, many patients can begin improving symptoms through smart food choices, portion control, and low-impact movement.

Key Fact: Every Pound Matters
Research suggests that for every pound of body weight lost, four pounds of pressure may be reduced across the knee during walking.
Small changes can make a meaningful difference.
Bracing for Knee Arthritis
How Knee Braces Can Help Manage Arthritis Pain
Knee braces can be a valuable nonsurgical tool that can provide support, reduce pain, improve stability, and help you stay active. They work by offering compression to control swelling, adding warmth for comfort, enhancing proprioception (your sense of joint position), and — in some cases — shifting weight away from the most damaged part of the joint.
Braces do not cure arthritis or reverse joint damage, but many patients find they make daily activities, walking, and exercise more comfortable. They are most effective when combined with exercise, weight management, and other strategies mentioned on this page.
Important note: Always consult with your doctor before starting to use a brace. The right choice depends on the location and severity of your arthritis, your activity level, and any knee instability
*All examples of braces listed below are popular examples patients often choose. The best choice depends on individual needs.
1. Knee Compression Sleeves
These are soft, slip-on sleeves (usually made of neoprene or elastic fabric) that provide gentle, all-around compression.
Benefits: Reduce swelling, provide warmth, improve proprioception, and give a sense of support and confidence during activity.
Best for: Mild to moderate arthritis, general aching, or activity-related discomfort.
Pros: Lightweight, easy to wear under clothing, affordable, and comfortable for all-day use.
Cons: Limited structural support; they do not correct alignment.
*Many patients start here because they are simple and effective for everyday use.
2. Hinged Knee Braces
These sleeves include metal or plastic hinges on the sides for added stability.
Benefits: Provide more support than a basic sleeve while still allowing natural knee movement. Helpful for mild instability or when the knee feels like it might “give way.”
Best for: Moderate arthritis with some ligament laxity or during higher-activity periods.
Pros: Good balance of support and mobility.
Cons: Slightly bulkier than sleeves.
3. Unloader (Offloading) Braces
These are more rigid, braces with hinges and straps that mechanically shift weight from the damaged compartment of the knee to the healthier side.
Benefits: Can significantly reduce pain during weight-bearing activities and may help delay the need for surgery in some patients with one-sided (unicompartmental) arthritis.
Best for: Moderate to severe arthritis affecting primarily the inner (medial) or outer (lateral) side of the knee.
Pros: Strongest evidence for pain relief among brace types for appropriate candidates. This includes localized pain and arthritis.
Cons: Larger, more expensive, and often require professional fitting, although over the counter options exist. Typically recommend having professional fit.




Supplements for Knee Arthritis
Can Supplements Help with Knee Arthritis?
Many patients ask about supplements as a natural way to support joint health, reduce pain, and improve function. While no supplement can cure arthritis or regrow cartilage, several have evidence showing they can provide meaningful relief when used alongside exercise, weight management, physical therapy, and other treatments we’ve discussed.
Supplements work best as part of a comprehensive plan. Results vary from person to person, and it often takes 8–12 weeks to notice benefits. It is typically recommended to use high-quality, third-party tested products.
Important Disclaimer: Supplements are not FDA-approved to treat arthritis. In fact, the AAOS listed the evidence as inconsistent, citing a need for additional research. Be sure to do your own research and always consult your doctor regarding possible interactions with medications.
*Below is a list of supplements most discussed with patients along with purchase options:
1. Curcumin (from Turmeric)
A potent anti-inflammatory compound.
Benefits: Reduces pain and stiffness; some studies show effects similar to NSAIDs with fewer side effects.
Typical Dose: 1,000–1,500 mg daily of a bioavailable form (e.g., with piperine, Meriva, or C3 Complex).
Best for: Daily inflammation and pain management.
Evidence: Strong — multiple meta-analyses support its use for knee osteoarthritis.
2. Boswellia Serrata (Frankincense extract, especially Aflapin or 5-Loxin)
A resin with powerful anti-inflammatory properties.
Benefits: Helps reduce pain, swelling, and improves function.
Typical Dose: 100–300 mg daily.
Best for: Patients seeking noticeable pain relief within weeks.
Evidence: Very strong for knee OA symptoms. Typically used in combination with Curcumin
3. Omega-3 Fatty Acids (Fish Oil or Krill Oil)
Benefits: Mild anti-inflammatory effects; supports overall joint comfort and heart health.
Typical Dose: 1,000–2,000 mg combined EPA + DHA daily.
Best for: Patients with mild-moderate symptoms or those who also want cardiovascular benefits.
Evidence: Moderate to good
4. Glucosamine Sulfate + Chondroitin Sulfate
Benefits: May support cartilage health and provide modest pain relief for some people.
Typical Dose: 1,500 mg glucosamine + 1,200 mg chondroitin daily.
Best for: Patients who prefer trying a traditional cartilage-support formula.
Evidence: Mixed — helpful for a subset of patients.
5. Collagen Peptides (Hydrolyzed or Undenatured Type II)
Benefits: Improves pain and function; may support joint tissue.
Typical Dose: 10 g daily (hydrolyzed) or 40 mg UC-II.
Best for: Longer-term joint support.
Evidence: Growing and promising.
6. Vitamin D
Benefits: Important for bone health, muscle strength, and may help reduce pain and improve function, especially if you are deficient (very common).
Typical Dose: 1,000–5,000 IU daily (or as directed by blood test results).
Best for: Anyone with low vitamin D levels or risk factors (limited sun exposure, older age, darker skin).
Evidence: Helpful for symptoms in deficient patients. Vitamin D Deficiency is a known cause of joint pain.






Injections for Arthritis
How Injections Can Help Manage Knee Arthritis
When conservative treatments like exercise, weight loss, physical therapy, and bracing are not enough, injections can provide targeted relief. These are performed in the office under sterile conditions.
Injections do not cure arthritis or regrow cartilage, but they can reduce pain, decrease inflammation, improve lubrication, or promote the body’s natural healing response. Results vary by individual, severity of arthritis, and the type of injection.
Important: All injections carry small risks (infection, bleeding, temporary pain flare). We review your medical history and use evidence-based techniques to minimize these risks.
1. Corticosteroid (Cortisone) Injections
A powerful anti-inflammatory medication injected directly into the knee joint.
• Benefits: Fast pain relief — often within a few days. Excellent for reducing swelling and managing flare-ups.
• How long it lasts: Typically 1–3 months (sometimes longer).
• Best for: Moderate to severe pain with significant inflammation, or when you need quick relief to participate in physical therapy.
• Pros: Quick acting, widely available, usually covered by insurance, low cost.
• Cons: Effects are temporary. Repeated use (more than 3–4 per year) may accelerate cartilage loss in some patients. Not ideal for long-term management.
Many patients use these occasionally for breakthroughs while continuing other treatments.
2. Hyaluronic Acid (Viscosupplementation) Injections
A gel-like substance (similar to natural joint fluid) that helps improve joint fluid properties, reduce inflammation, provide cartilage protective effects, as well as analgesic benefits.
• Benefits: Improves joint lubrication, reduces pain, and may improve function.
• How long it lasts: Relief often begins in 2–6 weeks and can last 3–6 months or longer in some patients.
• Best for: Mild to moderate arthritis, especially when pain is related to movement and stiffness.
• Pros: Generally very safe with low risk of serious side effects. Can be repeated as needed.
• Cons: Slower onset than cortisone. Results are variable — some patients respond very well, others notice modest improvement. Multiple injections (usually a series of 1–5) may be required depending on the product. Typically requires insurance authorization.
High-molecular-weight or cross-linked formulations tend to perform better in studies.

3. Platelet-Rich Plasma (PRP) Injections
Uses your own blood: we draw a small sample, concentrate the platelets (which contain growth factors), and inject them into the knee.
• Benefits: May reduce pain and inflammation while stimulating the body’s healing response. Growing evidence shows good results for pain and function.
• How long it lasts: Often 6–12 months or longer in responders.
• Best for: Mild to moderate osteoarthritis, patients seeking longer-term relief, or those who prefer a more “natural” biologic option.
• Pros: Autologous (from your own body), excellent safety profile, potential for longer-lasting benefits than steroids.
• Cons: More expensive, often not covered by insurance. Results vary, and multiple injections may be recommended. Takes longer to prepare and perform.
Recent studies suggest PRP often outperforms both cortisone and hyaluronic acid in mid- to long-term pain relief and function for many patients.
Physical Therapy for Knee Arthritis
Physical therapy (PT) is a cornerstone of nonsurgical knee arthritis management. The American Academy of Orthopedic Surgeons (AAOS) clinical practice guidelines provide a strong recommendation for supervised exercise management. Unlike medications or injections that mainly treat symptoms, PT addresses the root causes of pain and dysfunction by strengthening the muscles around the knee, improving joint stability, restoring mobility, and teaching you how to move with less pain.
Research shows that a well-designed physical therapy program can:
• Reduce pain as effectively as some medications
• Improve function and walking ability
• Delay or even avoid the need for surgery
• Increase confidence in daily activities
The best results come when PT is combined with weight management, bracing (when needed), and the other treatments discussed on this page.

What a Physical Therapy Program Typically Includes
Your physical therapist will create a personalized plan based on your specific arthritis severity, strength, and goals.
Common components include:
1. Strengthening Exercises
Strong muscles around the knee act as shock absorbers and take pressure off the joint.
• Focus areas: Quadriceps (especially vastus medialis), hamstrings, glutes, and calves.
• Examples: Straight leg raises, mini-squats, step-ups, clamshells, and bridge exercises.
• Goal: Build strength without aggravating the joint.
2. Range of Motion & Flexibility
Gentle stretching and mobility work help maintain or improve knee bending and straightening.
• Techniques: Heel slides, seated knee extensions, and gentle hamstring/quadriceps stretches.
3. Low-Impact Aerobic Exercise
Improves endurance and helps with weight control.
• Recommended: Stationary bike, elliptical, swimming, or walking with proper form.
4. Balance & Proprioception Training
Helps prevent falls and improves joint position sense.
• Examples: Single-leg stance, balance board work, or step exercises.
5. Manual Therapy & Modalities
Your therapist may use hands-on techniques (joint mobilizations, soft tissue massage) and tools such as ultrasound, electrical stimulation (TENS), or taping for short-term pain relief.
6. Education & Home Exercise Program
You’ll receive a customized home program so you can continue making progress between sessions. Learning proper movement patterns (e.g., how to go up/down stairs) is often one of the most valuable parts.
Using Medications Wisely as Part of Your Treatment Plan
Medications can be very helpful for controlling pain and inflammation in knee arthritis, allowing you to stay active and participate in physical therapy and exercise. However, medications treat symptoms rather than the underlying joint changes. The goal is to use the lowest effective dose for the shortest time necessary, while combining them with the other treatments on this page (exercise, weight loss, bracing, physical therapy, injections, and supplements).
It is important for an individualized medication plan based on your age, other medical conditions, kidney/liver function, and current medications.

Recommended Approach to Medication Management
Start with the safest, most effective options (often topical treatments + acetaminophen or short courses of NSAIDs).
Effective to aid with decreasing exacerbations
Some patients will use prior to athletic activities to decrease symptoms after exercise
Regular follow-up is important to monitor effectiveness and side effects.
Many patients are able to reduce or eliminate daily medications once they improve strength, lose weight, and establish a good exercise routine.
1. Acetaminophen (Tylenol)
Benefits: Reduces mild to moderate pain with a good safety profile when used correctly.
Typical Dose: Up to 3,000 mg per day (often 500–1,000 mg as needed).
Best for: Patients who cannot take anti-inflammatories or have mild symptoms.
Pros: Over-the-counter, generally well-tolerated.
Cautions: Do not exceed recommended dose (risk of liver damage, especially with alcohol use).
2. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
These are often the most effective oral medications for arthritis pain and swelling.
Oral NSAIDs (Ibuprofen, Naproxen, Meloxicam, etc.)
Benefits: Reduce both pain and inflammation.
Best for: Moderate pain with swelling or flare-ups.
Cautions: Stomach irritation, increased blood pressure, kidney effects, and heart risks with long-term use. Can be prescribed with stomach protection (e.g., omeprazole) when needed.
Topical NSAIDs (Diclofenac gel – Voltaren, Pennsaid)
Benefits: Excellent pain relief with much lower systemic absorption and fewer side effects.
Best for: Patients who want to avoid or cannot take oral NSAIDs.
3. Topical Treatments
Capsaicin cream: Helps reduce pain signals over time.
Lidocaine patches or creams: Numbs the area for temporary relief.
Best for: Localized pain with minimal side effects.
4. Other Prescription Medications
Duloxetine (Cymbalta): An antidepressant that also helps with chronic pain — often very useful for arthritis.
Tramadol: A milder opioid-like medication used occasionally for more severe pain.
Stronger opioids: Generally avoided for osteoarthritis due to risks and limited benefit.


Alternative Treatments
Coming Soon